
缺血性心肌病易与其他心肌病混淆 如何鉴别诊断?
2017-10-26 佚名 环球医学

59岁男性患者,因半个月前无明显诱因出现胸闷、气短、伴咳嗽入院,由超声心电图确诊为冠心病、陈旧性心肌梗死、缺血性心肌病。缺血性心肌病如何与扩张型心肌病鉴别诊断?临床中漏诊误诊的原因有哪些?详见病例要点——
59岁男性患者,因半个月前无明显诱因出现胸闷、气短、伴咳嗽入院,由超声心电图确诊为冠心病、陈旧性心肌梗死、缺血性心肌病。缺血性心肌病如何与扩张型心肌病鉴别诊断?临床中漏诊误诊的原因有哪些?详见病例要点——
病史和相关检查 患者,男性,59岁。半个月前无明显诱因出现胸闷、气短,活动耐量明显下降,气短夜间加重。平卧时有咳嗽,咯少量白色泡沫样痰。夜间有憋醒,坐起可缓解。3个月前无明显诱因出现胸骨后疼痛,持续约半天余。心电图示:Ⅰ、Ⅱ、Ⅲ、aVF、V4~V6异常Q波。
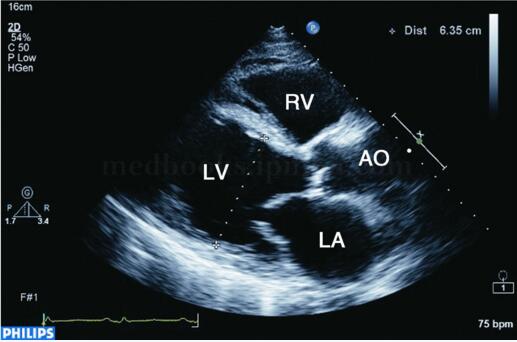
图2‐1‐178 左室长轴切面显示左心扩大,左室呈球形扩张
超声描述 左室下壁、后壁心肌变薄,约5mm,心肌回声增强,运动消失,其余节段心肌向心运动亦不同程度减弱,左心增大,左室略呈球形扩张,左室舒张末期内径63mm,左室泵血功能减低,左室EF32%。二尖瓣环扩张,探及中度二尖瓣反流。
超声诊断 左室下后壁心肌节段变薄、运动消失,其余节段运动减弱,符合缺血性心肌病改变,左室泵血功能减低,二尖瓣中度反流,提示乳头肌功能不全。
【讨论】
缺血性心肌病是由冠心病导致的严重心肌功能障碍,由于短暂或长期的心肌缺血,导致心肌功能障碍,心肌大面积纤维化,心室扩张,临床表现为心力衰竭。

图2‐1‐179 左室短轴切面显示下后壁心肌明显变薄,回声增强
常见超声表现
二维超声表现为左室显着扩大,几何形变,可呈球形扩张(见图2‐1‐179),左室心肌节段变薄,回声明显增强,运动明显减弱或消失,室壁增厚率消失,并伴有左室壁普遍运动减弱和不协调,左室泵血功能明显减低(见图2‐1‐180),二尖瓣开放幅度减低。左室腔内血流速度常较缓慢,有时可见附壁血栓形成。
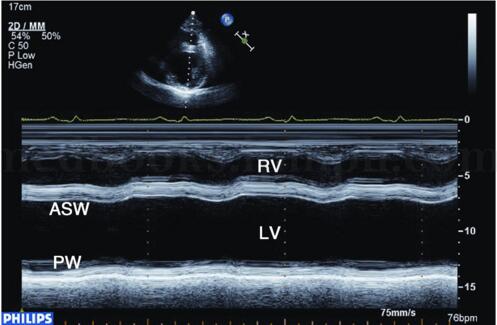
图2‐1‐180 M型超声显示左室后壁明显变薄,运动明显减弱甚至消失,前壁运动亦减弱
彩色和脉冲多普勒可探及多瓣口反流信号(图2‐1‐181)。连续多普勒测量舒张期二尖瓣血流E峰明显升高,A峰明显降低,E/A>2,EDT<140毫秒,提示左室充盈受限。连续多谱勒可探及三尖瓣反流速度加快,提示肺动脉压力升高。

图2‐1‐181 心尖四腔切面显示左室明显增大,彩色和脉冲多普勒探及二尖瓣中度反流信号(箭头)
鉴别诊断
扩张型心肌病 与缺血性心肌病同样表现为左心增大,左室呈球形扩张,左室收缩、舒张功能减低。不同点有:左室心肌无节段性变薄和回声增强,向心运动普遍减低。临床无冠心病病史,心电图和冠状动脉造影可帮助鉴别。
注意事项及误诊漏诊原因
缺血性心肌病多发生在慢性心肌缺血的病人,病程一般较长,伴有反复的心绞痛或心肌梗死病史,是冠心病终末的一种表现形式。多数病人常伴有明显的心肌功能障碍,对治疗不敏感。心脏超声检查时应注意评价室壁运动情况和运动协调性,并注意观察心腔内有无血栓形成。
版权声明:
本网站所有内容来源注明为“梅斯医学”或“MedSci原创”的文字、图片和音视频资料,版权均属于梅斯医学所有。非经授权,任何媒体、网站或个人不得转载,授权转载时须注明来源为“梅斯医学”。其它来源的文章系转载文章,或“梅斯号”自媒体发布的文章,仅系出于传递更多信息之目的,本站仅负责审核内容合规,其内容不代表本站立场,本站不负责内容的准确性和版权。如果存在侵权、或不希望被转载的媒体或个人可与我们联系,我们将立即进行删除处理。
在此留言
本网站所有内容来源注明为“梅斯医学”或“MedSci原创”的文字、图片和音视频资料,版权均属于梅斯医学所有。非经授权,任何媒体、网站或个人不得转载,授权转载时须注明来源为“梅斯医学”。其它来源的文章系转载文章,或“梅斯号”自媒体发布的文章,仅系出于传递更多信息之目的,本站仅负责审核内容合规,其内容不代表本站立场,本站不负责内容的准确性和版权。如果存在侵权、或不希望被转载的媒体或个人可与我们联系,我们将立即进行删除处理。
在此留言








#缺血性#
65
#鉴别诊断#
67
#缺血性心肌病#
117
#肌病#
76
超声应用越来越广泛.尤其是重症超声
104