
JNER:机器人训练有助于急性脑卒中患者运动功能恢复的生理机制
2021-09-12 MedSci原创 MedSci原创

中风后遗留的半身不遂,需要进行康复训练,才能使部分机体功能得到恢复。大约60%的患者在中风后6个月后依然无法恢复。到目前为止,已经有多种康复疗法,如运动疗法、镜像疗法、虚拟现实、神经-肌肉电刺激。此外
中风后遗留的半身不遂,需要进行康复训练,才能使部分机体功能得到恢复。大约60%的患者在中风后6个月后依然无法恢复。到目前为止,已经有多种康复疗法,如运动疗法、镜像疗法、虚拟现实、神经-肌肉电刺激。此外,机器人驱动装置在日常生活活动以及手臂和手的功能方面被证明是有效的。大多数评估机器人强化训练计划的研究都是在慢性中风患者中进行的。而且,关于机器人辅助治疗的影响以及中风后前3个月内瘫痪上肢的训练方法,研究较少。

康复的结果通常表现为运动功能改善。目前,对运动功能障碍和恢复的病理生理学的理解仍然有限。为了优化康复计划的设计,需要更全面地了解康复的生理过程。经颅磁刺激(TMS)作为安全无痛检查皮质和皮质脊髓生理学的合适工具,有助于解释这些过程。为了解决一些提出的问题,研究了亚急性中风患者上肢附加机器人辅助训练的效果。在训练中,使用了上肢外骨骼,提供可调节的手臂支撑,并允许重力支持和计算机增强的手臂练习(Armeo®Spring)。一些使用该装置的研究已经证明了运动功能的改善,包括力量的增加,以及痉挛和疼痛的减轻。本研究旨在回答三个问题:这种强化治疗会导致临床改善吗?额外的训练是否会引起运动兴奋性的变化?这些变化与运动功能的改善有何关系?在严重中风后较早期增加运动训练量是否可行,或者患者是否会因为过度疲劳而停止参与运动训练?本文发表在《Journal of NeuroEngineering and Rehabilitation》。

本研究是一项针对亚急性卒中后患者的前瞻性单盲病例对照研究。通过上肢Fugl-Meyer评估(FMA-UE)测量的上肢功能变化。测量运动诱发电位的大小和自愿性肌肉激活期间获得的皮层静默期的持续时间。进行行为任务和神经生理学实验并对其进行评分的研究人员对患者接受的训练类型是盲的。共有30名患有严重或中重度上肢偏瘫的亚急性中风患者被纳入研究。患者来自神经康复科(德国阿伦斯巴赫Kliniken Schmieder)。根据病例对照原则,将患者分为干预组或对照组。以基线FMA-UE值和患者年龄作为匹配标准。每组由15名参与者组成。

实验流程
机器人辅助治疗使用Armeo®Spring外骨骼,该外骨骼为上肢提供重量支撑,并连接到可玩各种虚拟现实游戏的PC。所有患者均参加常规住院神经康复治疗。重要的是,在住院患者康复期间,两组均接受低强度Armeo®Spring治疗(每周两次) × 30分钟),作为诊所标准康复程序内的治疗干预。干预组每周接受五次为期三周的额外45分钟的Armeo®Spring训练。常规的Armeo®治疗在下午进行,额外的培训课程在上午进行。
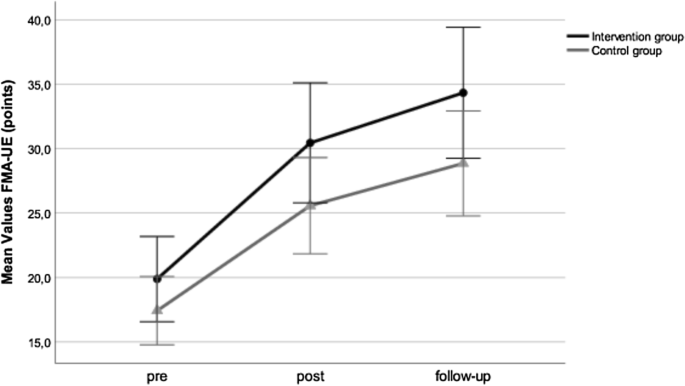
上肢Fugl-Meyer评估结果
为了记录运动功能的变化,患者在基线检查时、三周后(术后)和另外两周的住院康复(随访)后接受FMA-UE测试。选择两周的随访间隔(而不是三周或更长的时间)是为了最大限度地提高患者仍然可以作为住院患者接受检测的可能性。FMA-UE是中风后运动恢复的一种广泛使用的定量测量方法(分数范围为0-66;分数越高,表现越好)。功能改善5分或以上被认为是临床意义上的改变。在基线检查时采用Bells试验评估视空间忽视。该任务由一系列钟和无关的干扰物组成,并允许对视觉空间忽略进行定量评估。最高分是35分。
在25名受试者中,在基线检查时和3周后,使用连接到Magstim 200设备(英国Magstim有限公司)的圆形线圈在运动皮层上进行TMS测试。连续记录两个三角肌的运动诱发电位(MEP)和皮层静默期(cSP)。选择三角肌作为靶点的原因是期望从三角肌记录MEP和CSP的频率高于从手部肌肉记录。单次TMS脉冲用于测试皮质运动兴奋性。采用120%的运动阈值强度。两个大脑半球连续测试。给予五次刺激并计算平均值。记录是在受试者休息时进行的。在受试者以最大自愿收缩(MVC)的20%左右对三角肌进行等长收缩时,应用经颅磁刺激。首先,刺激未受影响的半球,然后刺激受影响的半球。连续给予五次刺激。通过测量从MEP开始到肌电活动再次出现的时间来分析cSP持续时间。对MEP振幅进行峰间测量。计算两个参数的平均值。MEP振幅被用作兴奋的指标,而cSP反映了抑制特性。
所有患者均未表现出失用症行为,也未表现出视觉空间忽视,且在认知上能够理解指令和执行任务。干预组的FMA-UE平均得分从基线检查到测试后提高了10.6分,从测试后到随访提高了3.9分。在对照组中,从基线检查到测试后,FMA-UE平均得分提高了7.3分,从测试后到随访,FMA-UE平均得分提高了3.3分。两组在FMA-UE方面均有显著改善(p < 0.001)。在三个时间点,各组之间均未观察到显著差异(p > 0.30)。13例患者中有10例FMA-UE值介于 10-20分达到了临床意义上的改善。FMA-UE值介于20-30分显示出5分或以上的变化。对照组的三名患者在治疗期间出现肩痛。因此,他们在后测试中恶化。相关分析显示基线FMA-UE与功能改善程度(rs)之间无显著相关性 = 0.22;p = 0.25)。
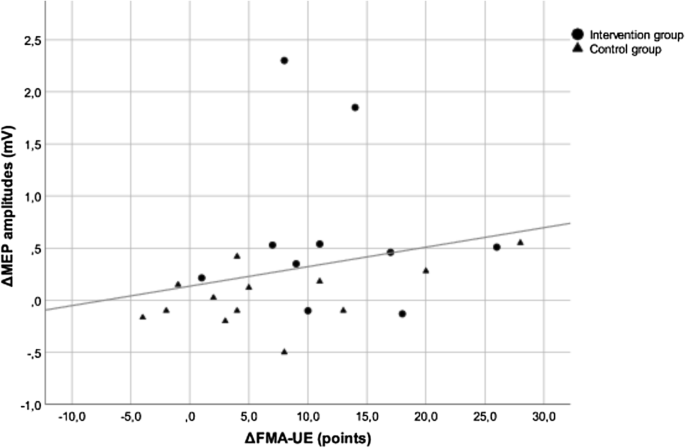
轻瘫侧预神经支配期间MEP振幅变化与临床改善程度之间的相关性
非瘫痪侧的神经生理学参数保持稳定,在术前、术后和组间比较中无显著差异(p > 0.05). 此外,两组受影响侧和健康侧在基线检查时的神经生理学参数存在显著差异(p < 0.002)。在21名患者中,受累半球的静息运动阈值超过刺激器输出强度的100%。因此,25名患者中有4名患者的MEP反应只能来自松弛的三角肌。三周后,可以从另外三名患者身上获得MEP反应。由于病例数量较少,未进行进一步的统计评估。基线检查时,除两名患者外,所有患者的瘫痪侧均可获得MEP。三周后,其中一名患者在神经支配前出现MEP。在干预组中,与试验前相比,试验后偏瘫侧的MEP振幅显著增加(p < 0.01)。 在对照组中,试验后与试验前相比,MEP振幅没有差异(p = 0.6)。 此外,两组在基线检查时没有差异(p = 0.44),但在测试后(p = 0.02). 干预组的MEP振幅显著高于对照组。
总之,在干预组中,额外的机器人辅助治疗导致更强的兴奋性增加。然而,这种效应并没有在行为水平上转化为运动性能的改善。
Sehle, A., Stuerner, J., Hassa, T. et al. Behavioral and neurophysiological effects of an intensified robot-assisted therapy in subacute stroke: a case control study. J NeuroEngineering Rehabil 18, 6 (2021). https://doi.org/10.1186/s12984-020-00792-1
本网站所有内容来源注明为“梅斯医学”或“MedSci原创”的文字、图片和音视频资料,版权均属于梅斯医学所有。非经授权,任何媒体、网站或个人不得转载,授权转载时须注明来源为“梅斯医学”。其它来源的文章系转载文章,或“梅斯号”自媒体发布的文章,仅系出于传递更多信息之目的,本站仅负责审核内容合规,其内容不代表本站立场,本站不负责内容的准确性和版权。如果存在侵权、或不希望被转载的媒体或个人可与我们联系,我们将立即进行删除处理。
在此留言













#运动功能#
58
#脑卒中患者#
60
#卒中患者#
53
#机器人#
64
#急性脑卒中#
57
#机器#
78
#功能恢复#
50
卒中虽然是临床上常见病,溶栓,取栓等血管内治疗也很成熟,但是仍然有很多未知问题有待认知!
72
机制研究离临床仍然有距离,不过与临床结合思考,仍然有帮助的,不能仅仅是纯临床思维,转化思维同样重要
89
卒中虽然是临床上常见病,溶栓,取栓等血管内治疗也很成熟,但是仍然有很多未知问题有待认知!
96