
蛛网膜下腔出血(SAH)指脑底部或脑表面的病变血管破裂,血液直接流入蛛网膜下腔引起的一种临床综合征,约占急性脑卒中的10%,是一种非常严重的常见疾病。WHO调查显示中国发病率约为2.0/10万人年。
SAH最常见的病因是颅内动脉瘤,典型临床表现为突然发生的剧烈头痛、恶心、呕吐和脑膜刺激征。剧烈活动中或活动后出现爆裂性局限性或全头部剧痛,难以忍受,呈持续性或持续进行性加重,有时上颈段也可出现疼痛。还可见因脑实质内,脑室出血等继发性SAH。

再出血是SAH的急性严重并发症,病死率约为50%左右。出血后24小时内再出血危险性最大,发病1个月内再出血的分先都较高。2周内再出血发生率为20%~30%,1个月为30%。其中,入院时昏迷、高龄、女性、收缩压超过170mmHg的患者再出血的风险较大。
目前,动脉瘤性蛛网膜下腔出血(aSAH)后的结果预测是一个挑战。据报道,CRP(C-反应蛋白)与预后有关,但不清楚上述关系是否独立于其他预测因素并适用于所有级别的aSAH。
为了评估CRP是否是aSAH后结果的独立预测因子,开发包含CRP的新预后模型,并测试这些模型是否可以通过应用机器学习来改进,近日,来自英国南开普敦总医院神经外科的专家开展了相关研究,结果发表在《卒中》Stroke杂志上。
研究人员对先前2项研究中SAH后72小时内患者的数据进行的个体患者层面的分析。包括逻辑回归、随机森林和支持向量机在内的一系列机器学习方法被用来评估CRP和改良Rankin量表(mRS)之间的关系。模型与完整的蛛网膜下腔出血国际试验者(SAHIT)预测蛛网膜下腔出血后结果的工具进行了比较,并使用交叉验证进行内部验证。

CRP用于SAHIT可提高预后的准确性
结果显示,共有1117名患者被纳入分析。总得来说,昏迷后第一天的CRP是一个独立的结果预测因子。完整的SAHIT模型的接受者特征曲线下面积(AUC)为0.831。逻辑回归预测结果显示,在完整的SAHIT模型的预测因素中加入CRP可以提高模型的性能(AUC=0.846, P=0.01)。
当使用随机森林(RF)进行学习时(AUC=0.807),上述改善没有得到加强。但进一步使用支持向量机(SVM)时(AUC=0.960,P<0.001)可在现有基础上进一步加强预测准确性。
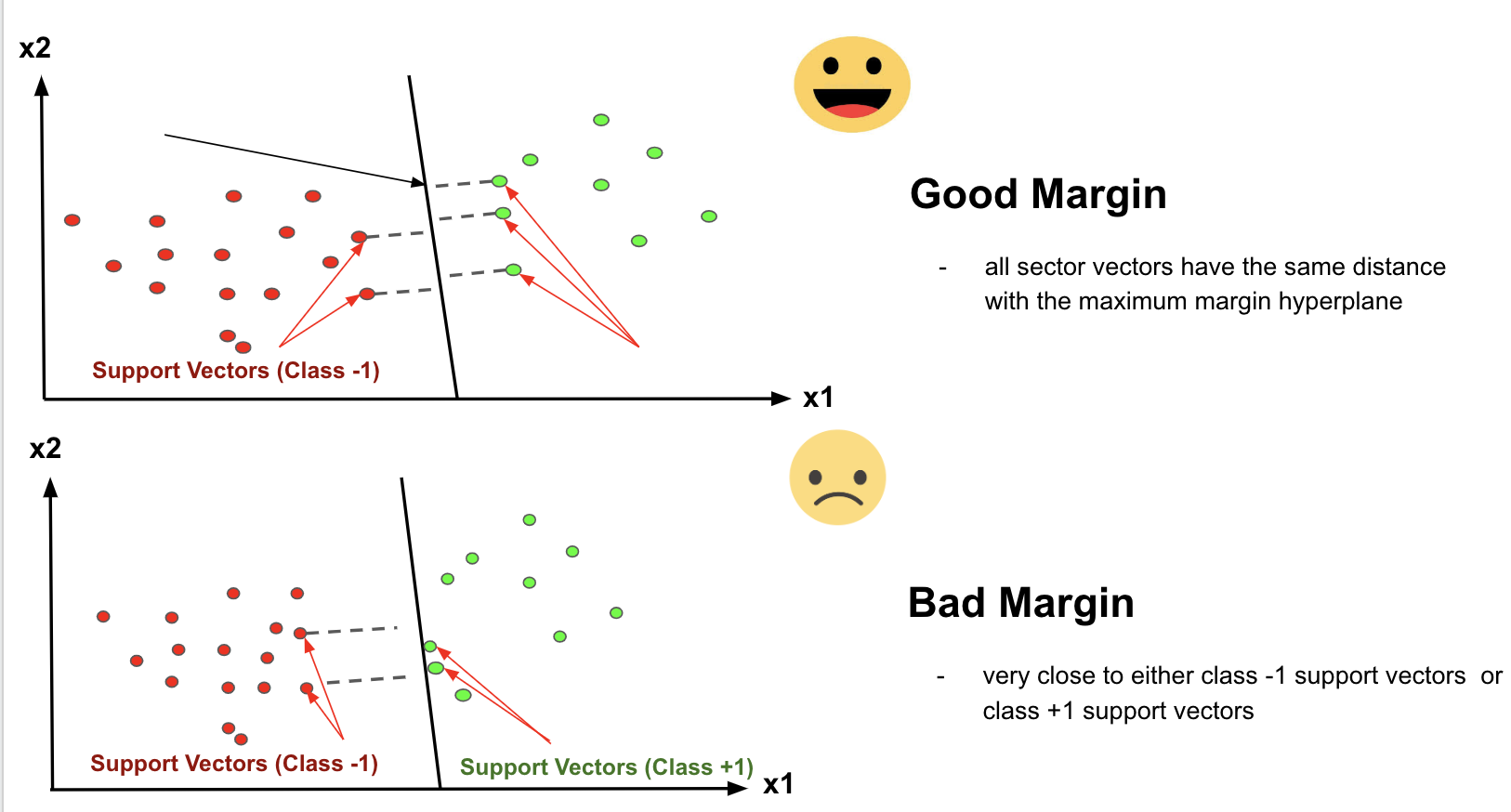
SVM工作原理示意图
由此可见,CRP是SAH预后的一个独立预测因素。将其纳入预后模型可以改善性能,尽管改善的程度可能不足以在临床上对个别病人产生影响,但在研究中更有意义。其中,支持向量机对模型性能的改善更大,但这些模型在内部验证中的分类错误率最高,需要外部验证和校准。
参考文献:
CRP (C-Reactive Protein) in Outcome Prediction After Subarachnoid Hemorrhage and the Role of Machine Learning.Stroke. ;0:STROKEAHA.120.030950 https://doi.org/10.1161/STROKEAHA.120.030950.
本网站所有内容来源注明为“梅斯医学”或“MedSci原创”的文字、图片和音视频资料,版权均属于梅斯医学所有。非经授权,任何媒体、网站或个人不得转载,授权转载时须注明来源为“梅斯医学”。其它来源的文章系转载文章,或“梅斯号”自媒体发布的文章,仅系出于传递更多信息之目的,本站仅负责审核内容合规,其内容不代表本站立场,本站不负责内容的准确性和版权。如果存在侵权、或不希望被转载的媒体或个人可与我们联系,我们将立即进行删除处理。
在此留言







#准确性#
73
#CRP水平#
44
#蛛网膜#
49
#CRP#
60
#机器#
47
谢谢 学习了
66