
磺脲类药物治疗2型糖尿病时若需添加SGLT-2抑制剂,可适当减少剂量以降低“低血糖”风险
2022-09-01 liangying MedSci原创

在磺酰脲类药物治疗中添加SGLT-2抑制剂时,适当减少磺酰脲类药物的剂量是很重要的,可以最小化低血糖风险并稳定疗效。
低血糖是降糖药常见的不良反应,与心血管疾病及死亡的风险增加有关。虽然血糖控制减少了糖尿病患者的心血管事件,但强化血糖控制既没有减少心血管事件,也没有降低2型糖尿病患者的全因死亡率。此外,来自糖尿病心血管风险控制行动(ACCORD)试验的数据表明,与标准治疗相比,强化治疗增加了全因死亡率和心血管死亡率,这可能与低血糖的负面影响有关。
当钠-葡萄糖共转运体2 (SGLT-2)抑制剂与磺酰脲类药物同时使用时,低血糖的风险并没有明确说明会增加。因此,有研究评估了与安慰剂和磺脲类药物相比,同时使用SGLT-2抑制剂和磺脲类药物的低血糖风险。

研究者搜索了Medline、EMBASE、Cochrane中心对照试验注册和Clinicaltrial.gov,找出了比较SGLT-2抑制剂与安慰剂治疗磺脲类2型糖尿病的随机试验。使用Cochrane工具评估每个试验的偏倚风险。低血糖风险比采用Mantel Haenszel法测定。此外,还进行了亚组分析来检验剂量效应。根据干预时间的长短,测量伤害所需数(NNH)。
最后纳入12项研究,包括3761名参与者,进行了相应的系统回顾和荟萃分析。结果发现,低血糖的风险比为1.67(95%CI 1.42-1.97)。在治疗持续时间为24周或更短的情况下,NNH为13(95%CI 9-21),在25至48周的情况下为11(8-18),在48周以上的情况下则为7(5-10)。
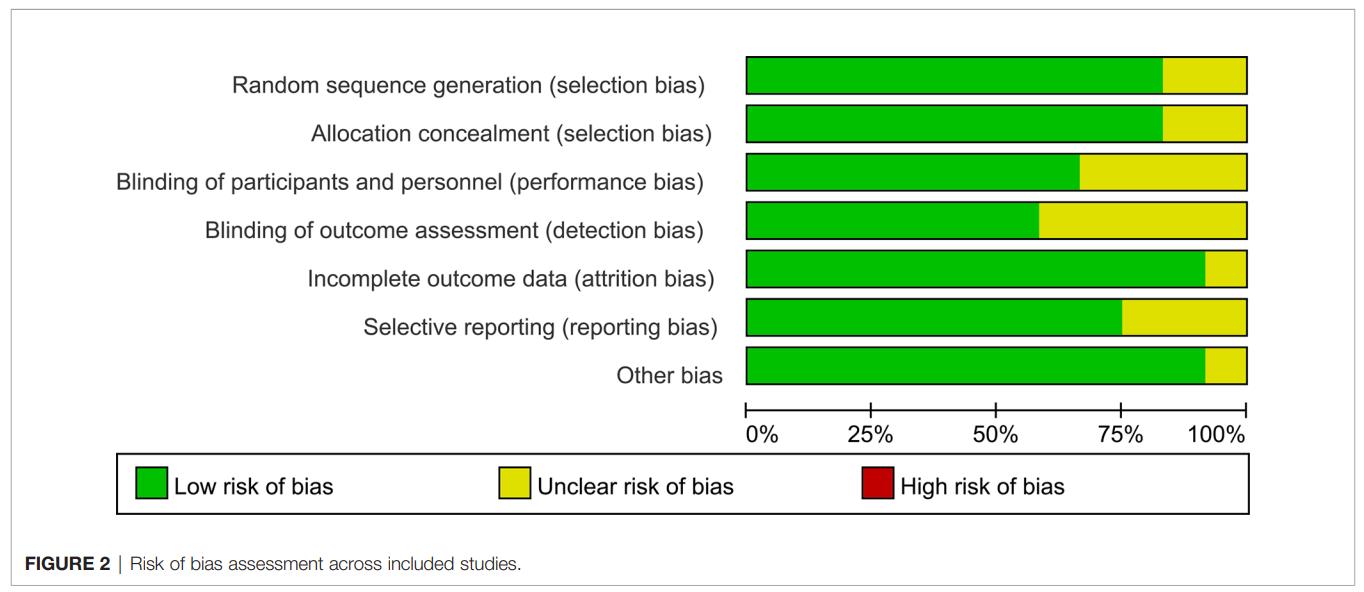
纳入研究的偏倚风险评估
亚组分析表明,高剂量和低剂量SGLT-2抑制剂之间没有差异。与低剂量SGLT-2抑制剂相关的风险比为1.56(95%CI 1.30-1.88),与高剂量SGLT-2抑制剂有关的风险比是1.70(95%CI1.42-2.04)。

SGLT-2抑制剂加磺脲类药物与安慰剂加磺脲类药物治疗的患者发生低血糖风险的森林图
该系统回顾和荟萃分析表明,当将SGLT-2抑制剂添加到磺脲类药物治疗糖尿病患者时,低血糖风险增加50%以上,并且这种联合治疗导致每13名患者在治疗持续时间少于治疗前6个月的情况下多发一例低血糖。
SGLT-2抑制剂增加葡萄糖排泄以降低高血糖,这是一种独特的胰岛素非依赖性作用模式,高血糖风险有限。由于SGLT-2抑制剂对心肾预后的有益影响,指南提出了一种糖尿病治疗的新模式——优先使用SGLT-2抑制剂。然而,在接受磺脲类药物治疗的患者中,胰岛素分泌已经独立于血糖水平而受到刺激,加之葡萄糖的消耗效应可能会导致低血糖发生率的增加。由于磺脲类药物的广泛使用和SGLT-2抑制剂在2型糖尿病治疗中的优先地位,联合治疗的风险将导致大量的诱导低血糖病例。
因此,研究者建议在使用SGLT-2抑制剂全剂量治疗时,可适当减少磺酰脲的剂量。此前,也有一项相关研究表明,在使用这种组合治疗的患者中,维持最低剂量的磺酰脲治疗可以确保更好的血糖控制,且不增加低血糖。然而,由于病例数量少和其他限制,需要进一步的研究来证实结。
总之,2型糖尿病患者在使用磺脲类类治疗方案时如添加SGLT-2抑制剂,可能会增加低血糖的风险。这种负面影响可能会导致世界范围内低血糖病例的再显著增加。这些结果强烈表明,在磺酰脲类药物治疗中添加SGLT-2抑制剂时,适当减少磺酰脲类药物的剂量是很重要的,可以最小化低血糖风险并稳定疗效。
参考文献:1.Jiang M, Liu Q, Jiang T, Nizigiyimana P, Lei M. Adding Sodium-Glucose Co-Transporter 2 Inhibitors to Sulfonylureas and Risk of Hypoglycemia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front Endocrinol (Lausanne). 2021 Oct 21;12:713192. doi: 10.3389/fendo.2021.713192.
2.Takahashi K, Cho KY, Nakamura A, Miya A, Miyoshi A, Yamamoto C, et al.. Should Sulfonylurea Be Discontinued or Maintained at the Lowest Dose When Starting Ipragliflozin? A Multicenter Observational Study in Japanese Patients With Type 2 Diabetes. J Diabetes Investig (2018). doi: 10.1111/jdi.12913

本网站所有内容来源注明为“梅斯医学”或“MedSci原创”的文字、图片和音视频资料,版权均属于梅斯医学所有。非经授权,任何媒体、网站或个人不得转载,授权转载时须注明来源为“梅斯医学”。其它来源的文章系转载文章,或“梅斯号”自媒体发布的文章,仅系出于传递更多信息之目的,本站仅负责审核内容合规,其内容不代表本站立场,本站不负责内容的准确性和版权。如果存在侵权、或不希望被转载的媒体或个人可与我们联系,我们将立即进行删除处理。
在此留言









#2抑制剂#
99
#SGLT-2抑制#
78
#SGLT#
52
#抑制剂#
51
#SGLT-2#
75
#磺脲类#
89
这个相当有意思,在#糖尿病#中,大家知道,#磺脲类药物#降糖是很强的,只是大家会顾虑其#低血糖#的安全性问题,但是,这里联合#SGLT-2抑制剂#,如#恩格列净##达格列净#,这样既保证能深度降糖,同时还具有较好的安全性,这确实是一种选择!
128