
消化性溃疡(PU)诊疗,基础必备!
2021-12-18 陈飞帆 纷飞之翼之住院医师学习笔记 陈飞帆 纷飞之翼之住院医师学习笔记

消化性溃疡是各种致病因子导致黏膜炎性坏死,形成溃疡,缺损穿透黏膜肌层,严重者可达固有肌层,可发生于食管、胃或十二指肠,以胃十二指肠最常见。
1、概述
-
定义:各种致病因子导致黏膜炎性坏死,形成溃疡,缺损穿透黏膜肌层,严重者可达固有肌层 -
可发生于食管、胃或十二指肠,以胃十二指肠最常见 -
以20-50岁居多,男:女(2-5):1,十二指肠溃疡:胃溃疡3:1
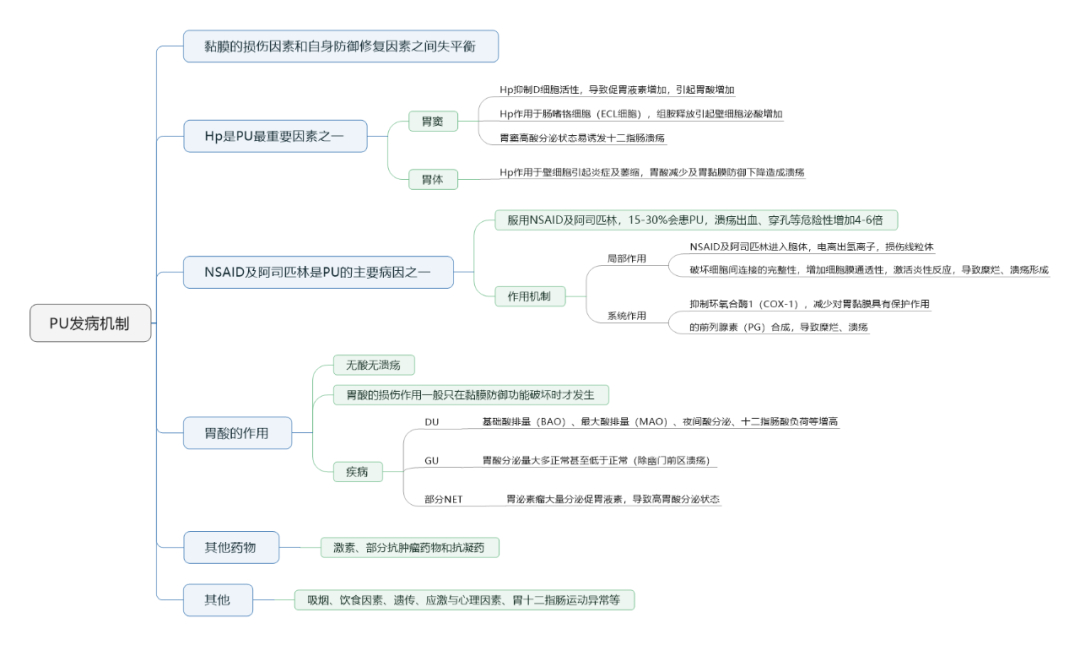
2、发病机制
3、诊断及鉴别
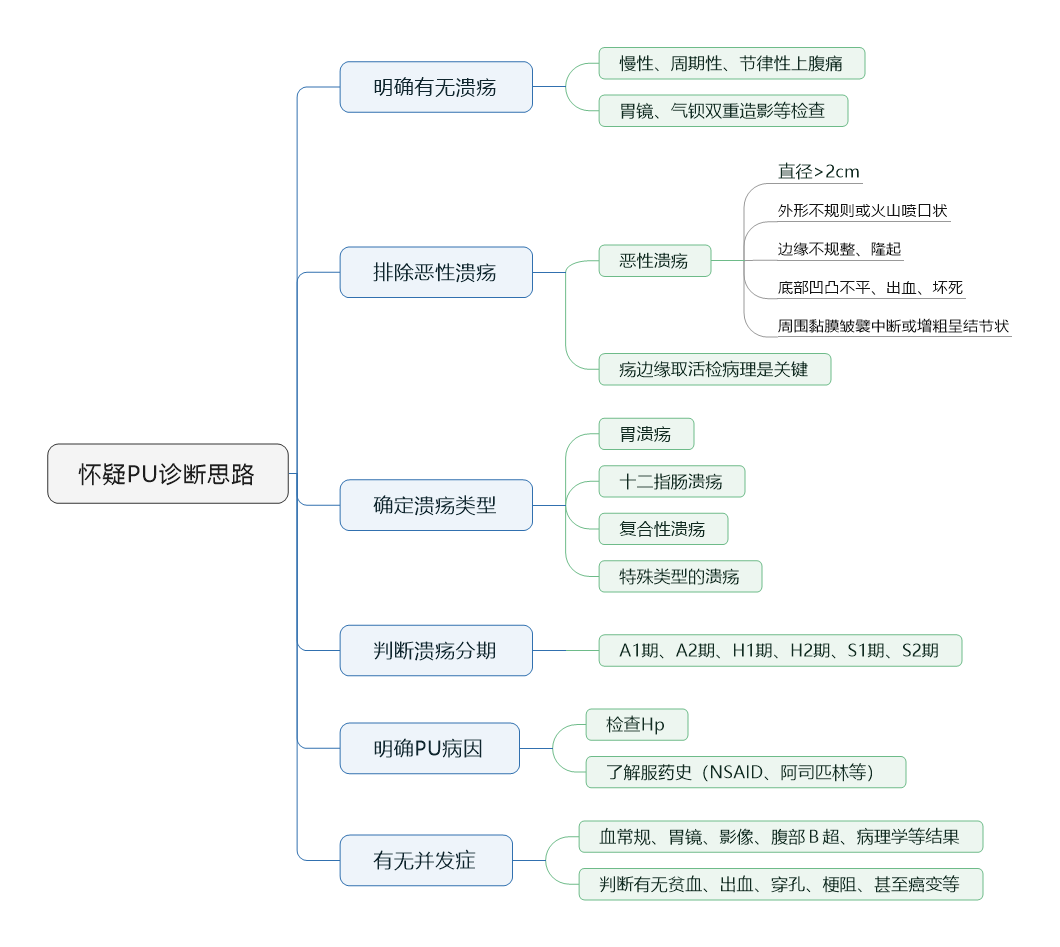
(1)诊断思路
-
中上腹痛,周期性、节律性发作 -
胃溃疡腹痛:餐后0.5-1h -
十二指肠溃疡腹痛:空腹 -
NSAIDs溃疡 -
无症状者居多 -
部分以上消化道出血为首发症状 -
或恶心、厌食、纳差、腹胀等非特异症状
-
胃镜 -
诊断PU最主要方法,注意部位、形态大小、深度、病期,以及周围黏膜情况 -
胃溃疡应常规活检,治疗后应复查胃镜至溃疡愈合 -
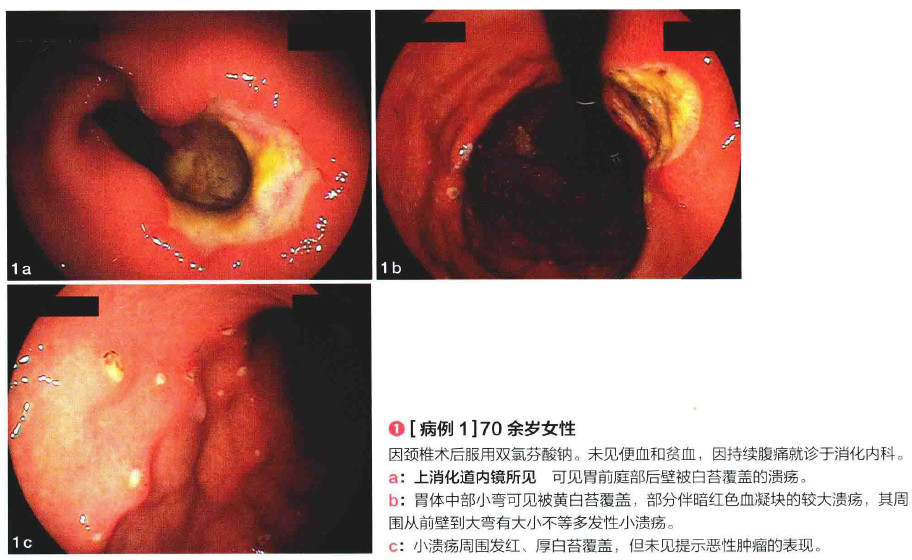
NSAIDs溃疡 -
胃窦、胃体、胃角等不同部位,形态多样,大小不一,常呈多发、浅表性溃疡
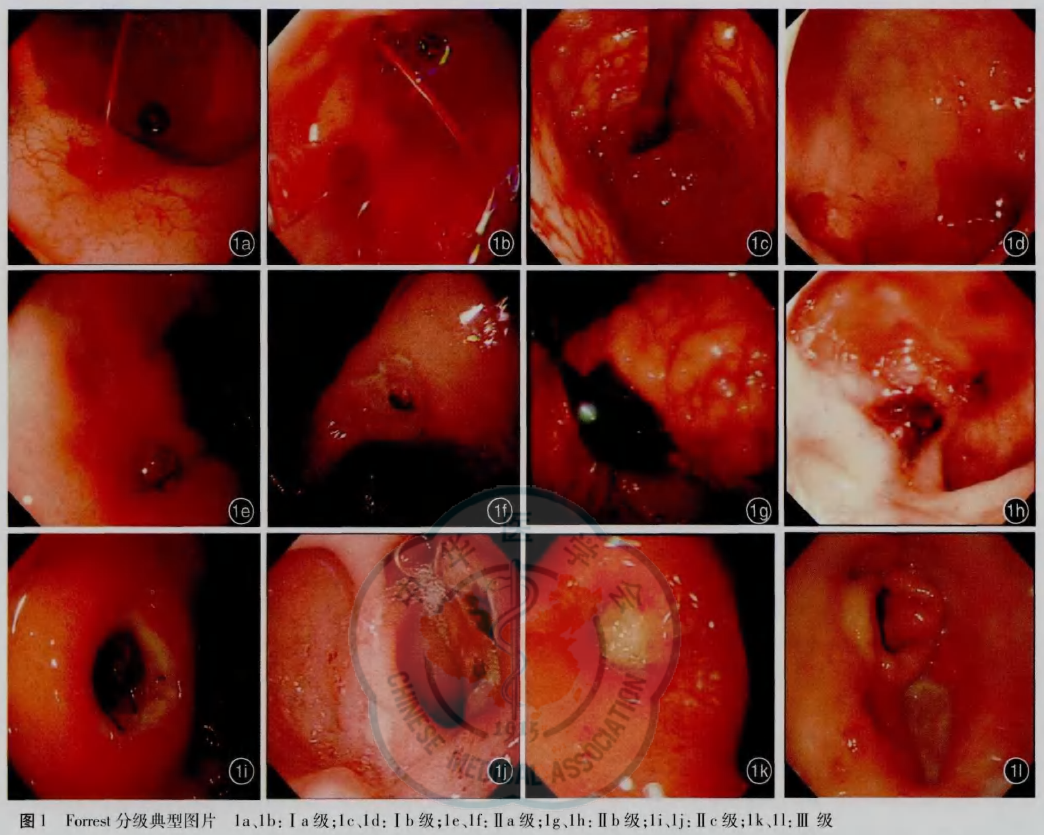
 PU出血Forrest分级
PU出血Forrest分级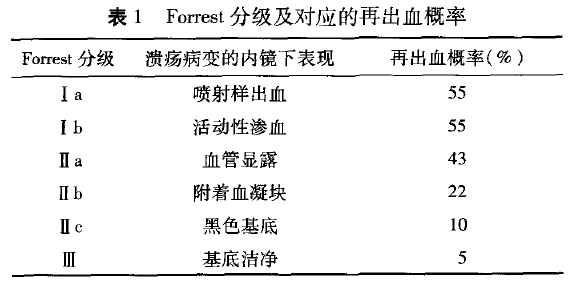
 PU内镜分期
PU内镜分期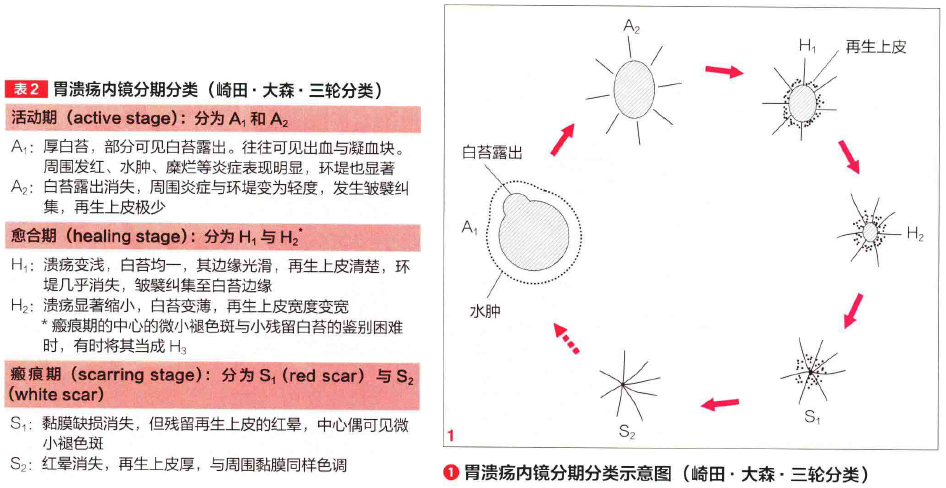
-
不典型或难愈合溃疡 -
应进一步完善胃肠钡餐、超声内镜、共聚焦内镜等 -
HP检查 -
PU常规做尿素酶试验、组织学检测,或核素标记C13/14呼气试验 -
粪便抗原检测:准确性与呼气试验相似 -
细菌培养:用于药物敏感试验和细菌学研究 -
血清抗体检测:只适用于普查,不能分辨是否为现症 -
注: -
抗菌药物、铋剂停药至少4周后进行检测 -
应用抑酸剂停药至少2周后进行检测 -
PU出血,严重萎缩,MT可能导致尿素酶试验假阴性 -
病理提示活动性炎性反应高度提示HP+ -
活动性PU排除NSAID溃疡后,Hp感染可能>95%
-
MT、MALT、CD、TB、CMV感染等
-
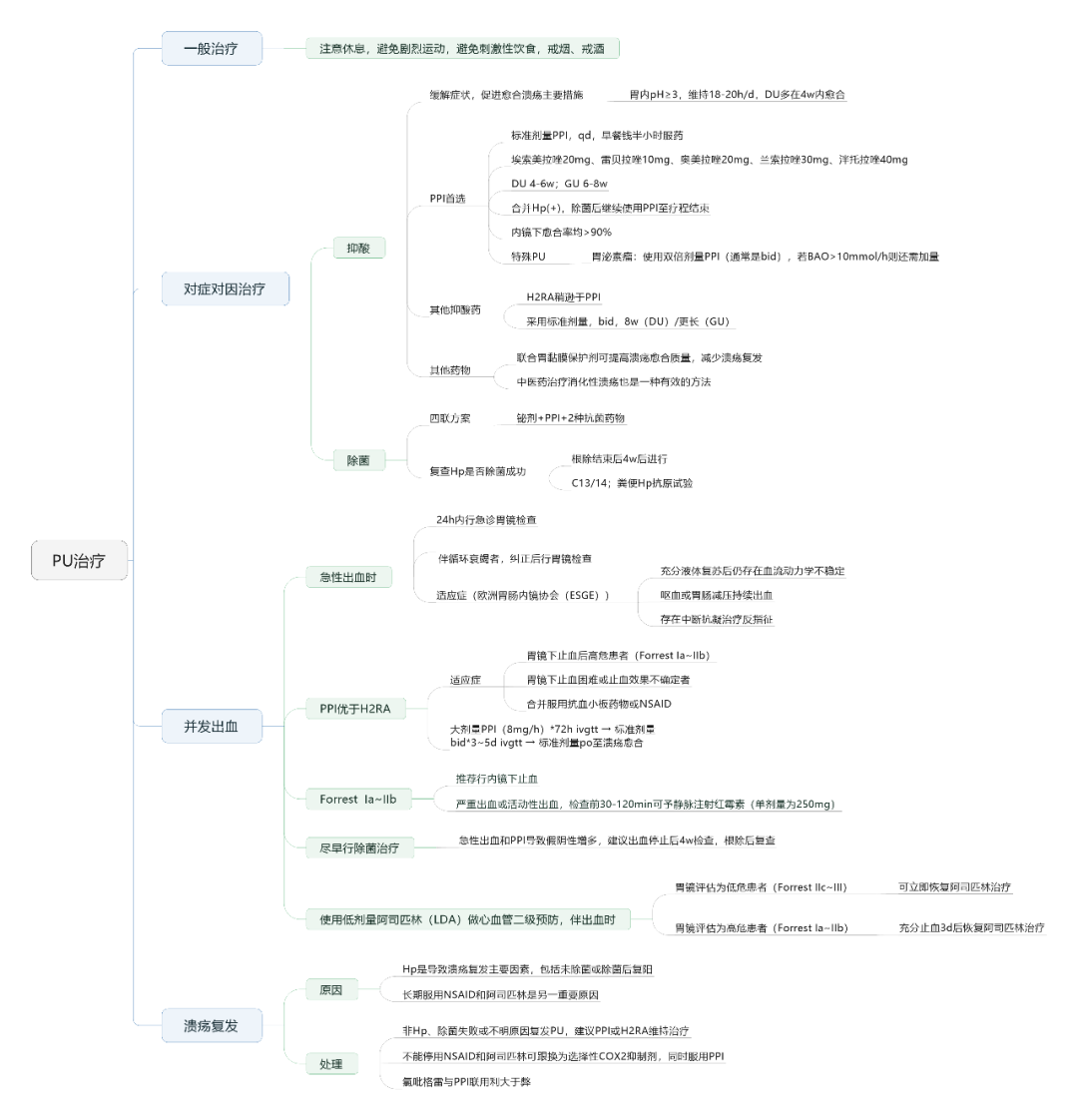
病情允许的情况下,首选停用NSAID -
药物 -
PPI是治疗首选药物,预防出血,促进溃疡愈合 -
胃黏膜保护剂可增加前列腺素合成,对NSAID溃疡有一定作用 -
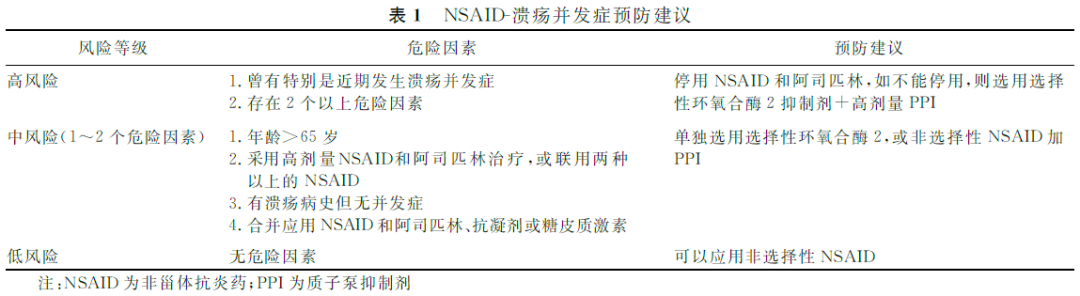
并发症 -
风险分级及处理
-
预防 -
患者既往无PU史,仍推荐抑酸以预防低剂量阿司匹林(LDA)相关溃疡的发生 -
除菌:存在争议 -
部分认为长期接受NSAID和阿司匹林治疗根除Hp有益 -
另外部分认为使用PPI疗效优于除菌,且除菌不加速溃疡愈合
小提示:本篇资讯需要登录阅读,点击跳转登录
版权声明:
本网站所有内容来源注明为“梅斯医学”或“MedSci原创”的文字、图片和音视频资料,版权均属于梅斯医学所有。非经授权,任何媒体、网站或个人不得转载,授权转载时须注明来源为“梅斯医学”。其它来源的文章系转载文章,或“梅斯号”自媒体发布的文章,仅系出于传递更多信息之目的,本站仅负责审核内容合规,其内容不代表本站立场,本站不负责内容的准确性和版权。如果存在侵权、或不希望被转载的媒体或个人可与我们联系,我们将立即进行删除处理。
在此留言
本网站所有内容来源注明为“梅斯医学”或“MedSci原创”的文字、图片和音视频资料,版权均属于梅斯医学所有。非经授权,任何媒体、网站或个人不得转载,授权转载时须注明来源为“梅斯医学”。其它来源的文章系转载文章,或“梅斯号”自媒体发布的文章,仅系出于传递更多信息之目的,本站仅负责审核内容合规,其内容不代表本站立场,本站不负责内容的准确性和版权。如果存在侵权、或不希望被转载的媒体或个人可与我们联系,我们将立即进行删除处理。
在此留言










谢谢
70
学习
129
#消化性溃疡#
82
学习了,C13与粪便抗原检测准确性相似,一直被误解了!
95
学习学习学习学习学习学习学习学习学习学习学习学习学习学习学习学习学习
130
简单,全面,前卫。
83