左臀部肌上皮癌超声表现1例
2019-10-19 吴翠怡 吴佳偿 冯宁娜 临床超声医学杂志

患者女,27岁,因“左臀部肿物3个月,增大伴疼痛2个月余”入院。体格检查:左臀部见一大小约10 cm×8 cm×5 cm肿物,压痛(+),皮下波动感(-)。超声检查:左侧臀部皮下脂肪层内见大小约114mm×45mm团状不均匀低回声,边界尚清,形态不规则,呈分叶状改变,内见少许不规则片状无回声区,后方回声增强,与后方骨皮质分界欠清;CDFI示其内及周边见点条状血流信号,收缩期峰值流速42.8 cm/
患者女,27岁,因“左臀部肿物3个月,增大伴疼痛2个月余”入院。体格检查:左臀部见一大小约10 cm×8 cm×5 cm肿物,压痛(+),皮下波动感(-)。超声检查:左侧臀部皮下脂肪层内见大小约114mm×45mm团状不均匀低回声,边界尚清,形态不规则,呈分叶状改变,内见少许不规则片状无回声区,后方回声增强,与后方骨皮质分界欠清;CDFI示其内及周边见点条状血流信号,收缩期峰值流速42.8 cm/s,阻力指数0.88(图1)。超声诊断:左侧臀部皮下实性占位,性质待定。
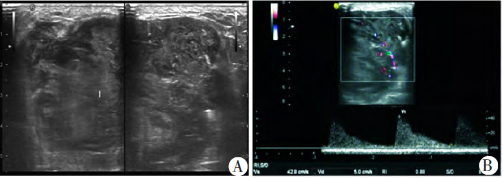
图1 左臀部肿物声像图。A:二维声像图;B:血流频谱图。
术中见肿物位于皮下组织层内,与肌肉分界尚清,包膜尚完整,呈囊实性,伴囊内出血,坏死鱼肉样。免疫组化检查:EMA灶性+,S100+,Myogenin+,Calpoint+,Ki67+(60%),CK-,SMA-,myoD1-,P63-,Des-,INI-1-,Bc12-,CD99-,CD34-。术后病理结果:考虑为软组织来源的高级别恶性肿瘤。
结合免疫组化结果符合肌上皮癌。患者术后恢复良好,于外院行辅助性放疗25次,复查未见复发或转移。
讨论:
肌上皮癌主要源自腮腺。与唾液腺肌上皮癌比较,软组织肌上皮癌更为罕见。软组织肌上皮癌大体形态特征一般为边界清楚,呈分叶状,但常表现为浸润性生长,可能存在出血和坏死,最常见于四肢,也见于头颈部、躯干及内脏软组织,发生于臀部者较少报道;好发于30~50岁,男女发病相等。临床多表现为无痛性肿块,迅速增大者可伴有疼痛,本例患者亦是如此。该病确诊主要依靠免疫组化检查。由于本例患者发病部位为臀部皮下软组织,位置较表浅,超声可作为首选检查方法。
应用彩色多普勒超声可以描述病变范围、形态、毗邻关系及血流特点,从而明确病变性质。本例病变边界尚清,形态呈分叶状与其大体形态相似,而内部回声不均匀、形态不规则及高速高阻血流特点,均提示其恶性可能性大,另外出现后方回声增强,考虑与病灶出血、坏死有关。由于本例病变体积较大,所以超声对其后方显像不清,表现为与后方骨皮质分界欠清。该病需与软组织肉瘤相鉴别,后者可出现明显骨质破坏。超声对临床了解病变的位置、形态、血流等有一定的临床价值。
原始出处:
吴翠怡,吴佳偿,冯宁娜.左臀部肌上皮癌超声表现1例[J].临床超声医学杂志,2018(05):345.
版权声明:
本网站所有内容来源注明为“梅斯医学”或“MedSci原创”的文字、图片和音视频资料,版权均属于梅斯医学所有。非经授权,任何媒体、网站或个人不得转载,授权转载时须注明来源为“梅斯医学”。其它来源的文章系转载文章,或“梅斯号”自媒体发布的文章,仅系出于传递更多信息之目的,本站仅负责审核内容合规,其内容不代表本站立场,本站不负责内容的准确性和版权。如果存在侵权、或不希望被转载的媒体或个人可与我们联系,我们将立即进行删除处理。
在此留言
本网站所有内容来源注明为“梅斯医学”或“MedSci原创”的文字、图片和音视频资料,版权均属于梅斯医学所有。非经授权,任何媒体、网站或个人不得转载,授权转载时须注明来源为“梅斯医学”。其它来源的文章系转载文章,或“梅斯号”自媒体发布的文章,仅系出于传递更多信息之目的,本站仅负责审核内容合规,其内容不代表本站立场,本站不负责内容的准确性和版权。如果存在侵权、或不希望被转载的媒体或个人可与我们联系,我们将立即进行删除处理。
在此留言




#超声表现#
77
#肌上皮癌#
71
#臀部#
75
#上皮癌#
63