
多中心真实世界研究:基于血浆ctDNA突变的转移性乳腺癌亚型临床分析
2022-07-30 测序中国 测序中国

该研究依据传统的HER2/HR的状态对乳腺癌患者进行分层治疗,但经过多线治疗后,传统基于免疫组化的HER2/HR的状态不能指导转移性乳腺癌的患者治疗。
循环肿瘤DNA(ctDNA)由肿瘤细胞死亡后释放到体循环中,理论上是来自不同转移部位的肿瘤DNA混合物,可以充分体现肿瘤的异质性。因此ctDNA可以作为mBC患者监测临床预后和治疗疗效的指标,并可根据ctDNA特定的变异指导mBC患者的后线治疗。
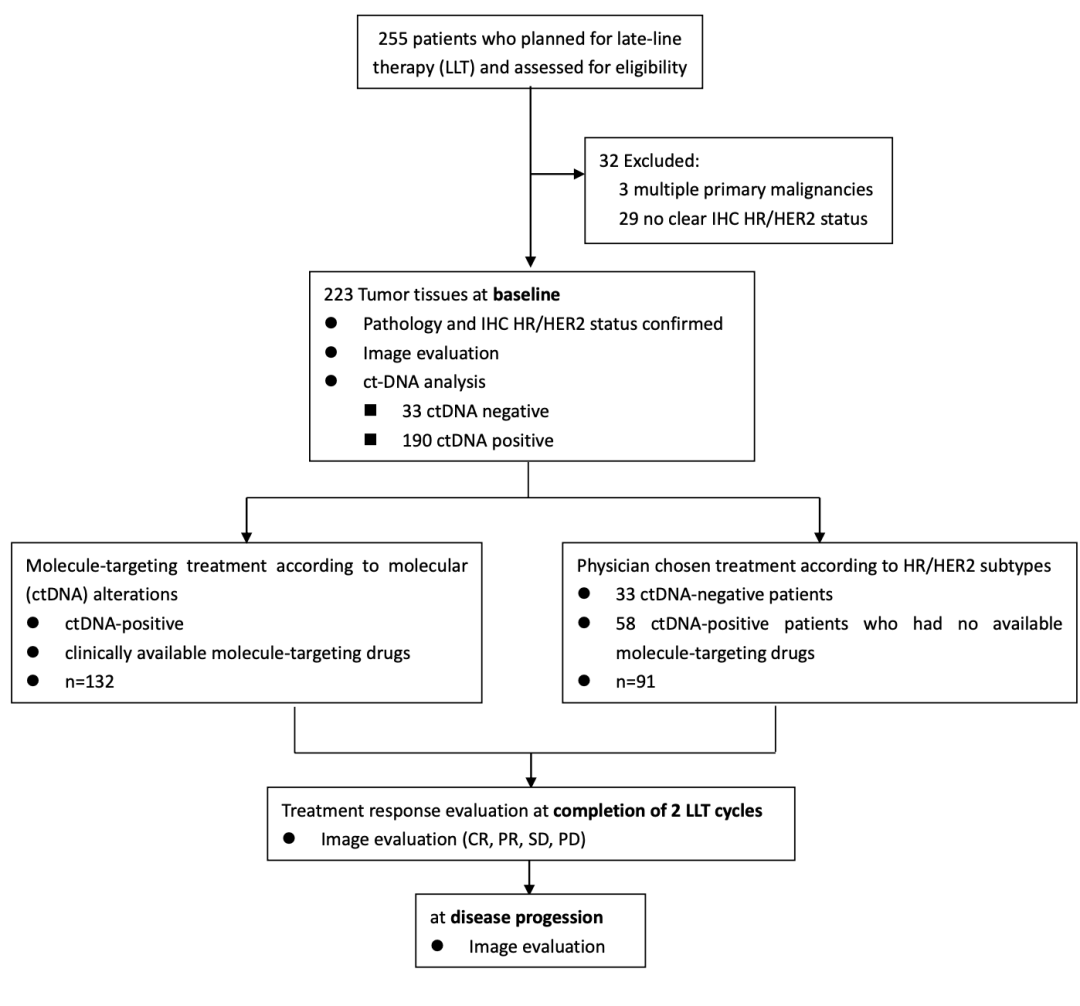
图1. 分组临床设计方法
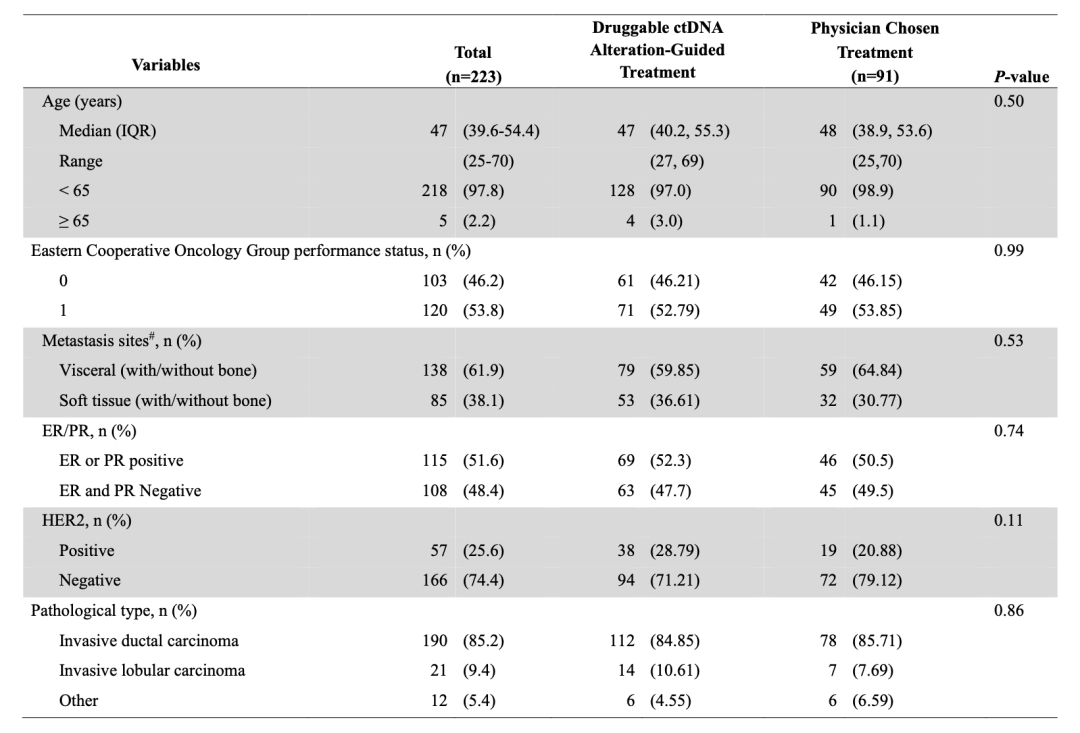
表1. 入组人群的基本特征
研究结果
1. 转移性乳腺癌ctDNA变异图谱
在参加该试验的223例患者中,190例患者(85%)在基线ctDNA被检出阳性,此外有132例患者(69.5%)检测到了可以提示临床靶向治疗的ctDNA 突变。研究结果显示,频繁突变的基因是TP53、PIK3CA、ERBB2、BRCA1、ESR1、CDK12和FGFR。除TP53外,其它基因变异均存在相关药物。(图2)
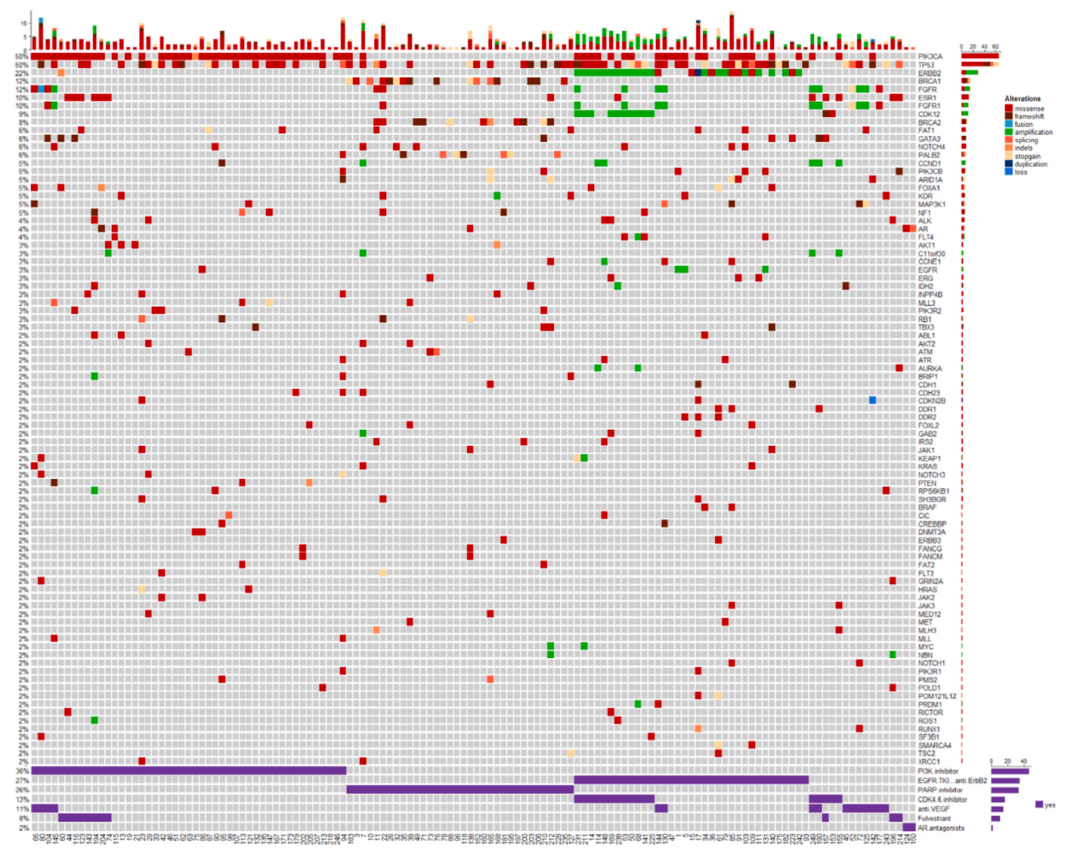
图2. ctDNA变化图谱
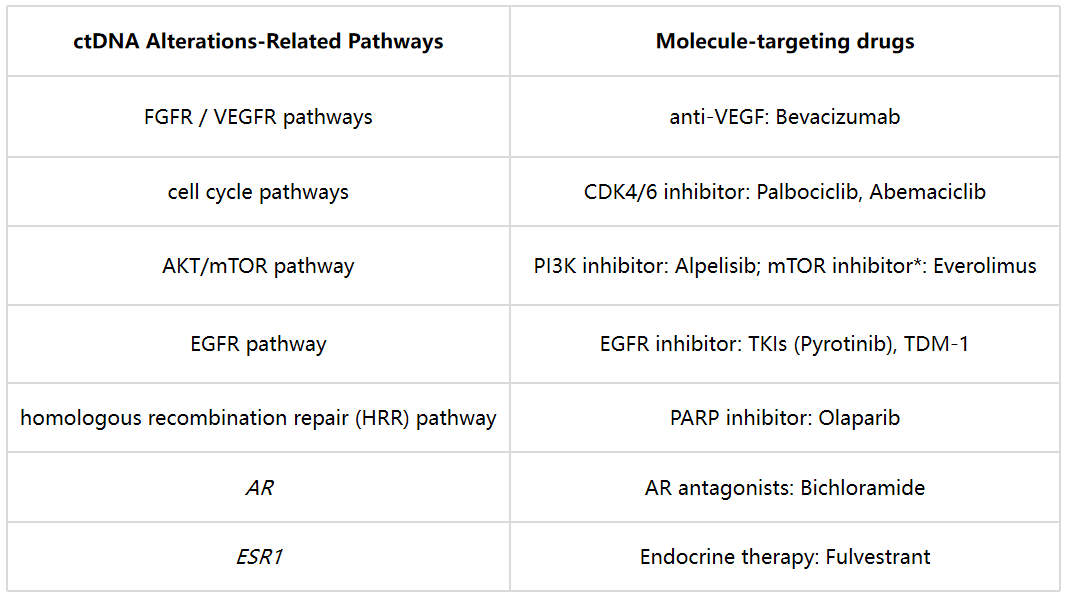
如下表所示(表2),具有FGFR/VEGFR突变的患者接受抗VEGFR/FGFR抑制剂单用或者联合化疗治疗,具有影响细胞增殖突变的患者使用细胞周期蛋白依赖性激酶4/6抑制剂(Cyclin-dependent kinase 4/6 inhibitor, CDK4/6i)治疗;具有同源重组修复(homologous recombination repair, HRR)通道突变的患者,接受PAPR抑制剂(PAPRi)治疗;具有PI3K/mTOR通路基因相关突变的患者接受PI3K/mTOR抑制剂治疗。结果显示,该研究发现绝大部分ctDNA阳性患者存在药物相关的基因变异,可用于指导临床用药。
表2. 不同突变类型的患者用药方案
2. DDAT组有更高的疾病控制率和无病进展生存期
经过两个治疗疗程后,通过影像学的方式对223例患者进行临床疗效评估(图3)。总体而言,45例患者疾病进展(PR), 92例患者疾病稳定(SD), 86例患者部分缓解(PR),疾病控制率(DCR)高达79.8%。在ctDNA指导治疗组(DDAT)中,89.4%的患者肿瘤PR或SD(118例),但是医师决策治疗组(PCT)中仅65.9%的患者PR或SD(60例),DDAT组有显著的临床获益(P<0.0001)。
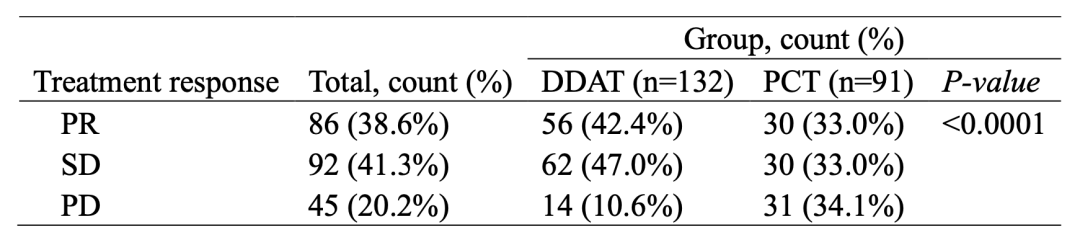
图3. 223名患者临床疗效评估
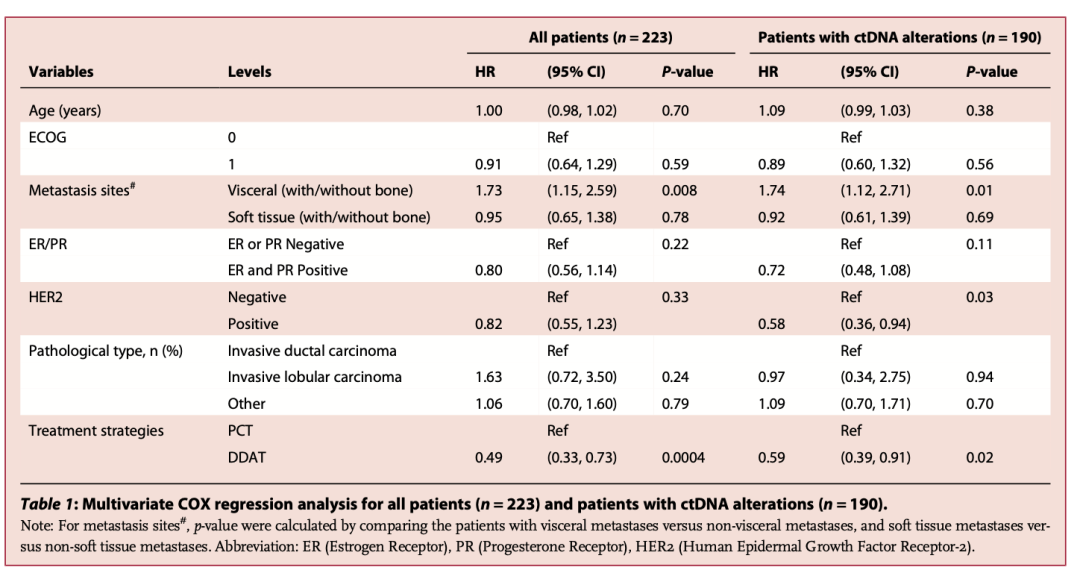
根据治疗策略进行亚组分析,生存曲线分析结果显示DDAT组的患者相较PCT组的患者具有更长PFS(6.3 vs 4.3 月,P<0.001)(图4)。此外,DDAT组的患者相较PCT组ctDNA阳性但是缺乏可用药物的患者同样具有更长PFS(6.3 vs 4.7月,HR: 0.56, 95%CI: 0.38-0.82, P=0.003)(图5)。COX分析结果也同样表明DDAT组的患者风险比显著低于所有PCT组的患者(HR:0.49, 95%CI: 0.33-0.73, P=0.0004)和PCT组ctDNA阳性但是缺乏可用药物的患者(HR:0.59, 95%CI: 0.39-0.91, P=0.02)(表3)。上述结果均表明,利用ctDNA检测存在药物靶点的患者的临床获益好于PCT组的患者。
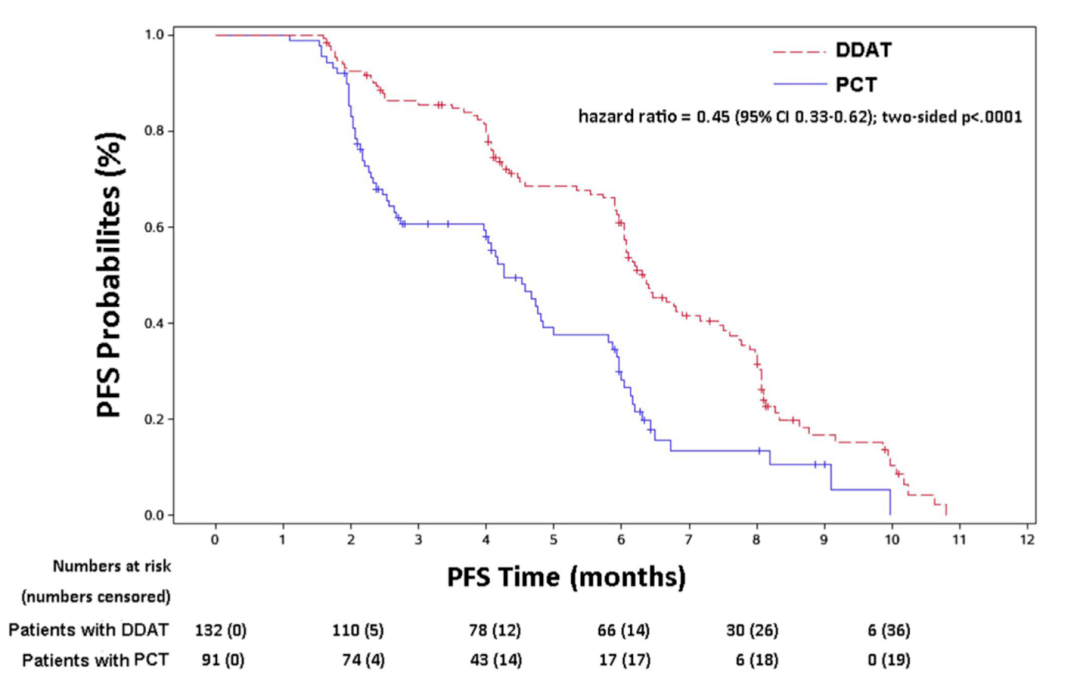
图4. DDAT组的患者较于PCT组的患者具有更长PFS
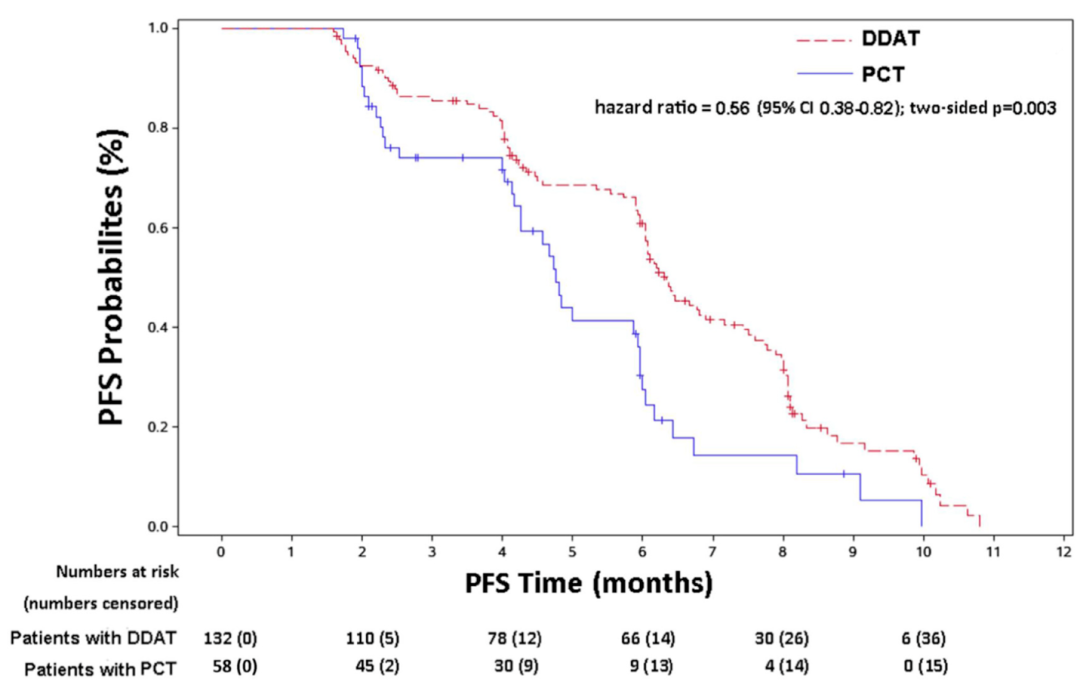
图5. DDAT组的患者较于PCT组ctDNA阳性但是缺乏可用药物的患者同样具有更长PFS
3. 不同分子亚型的转移性乳腺癌临床获益
为了阐明不同的分子亚型对转移性乳腺癌临床获益的影响,该研究利用层次聚类的方法对223例患者的ctDNA结果进行聚类。研究结果表明,mBC的基因变异可以分成4种亚型,分别是subtype 1(extracellular function,ECF同血管生成相关)subtype 2(cell proliferation, CP, 细胞增殖相关),subtype 3(nuclear function, NF, DNA修复相关)和 subtype 4(cascade signal pathway, CSP, PI3K/mTOR, MAPK等信号代谢通路相关)。
为了评估不同的分子亚型对PFS临床获益的影响,该研究采用单因素COX分析的方法,其结果如下图所示。subtype 3亚型(NF)的患者相较于PCT的患者获得了显著获益(HR:0.394, 95% CI 0.238-0.652, P=0.0003),同时,subtype 4亚型(CSP)的患者较于PCT患者获得了更好的临床获益(HR:0.142, 95% CI 0.094-0.215, P<0.0001)(图6)。但subtyple1(ECF)和subtype 2(CP)亚型没有获得显著的临床获益(P>0.05)。上述结果表明,DDAT组中特别是具有能够影响信号通路和DNA修复变异的患者能够获得更好的临床获益。
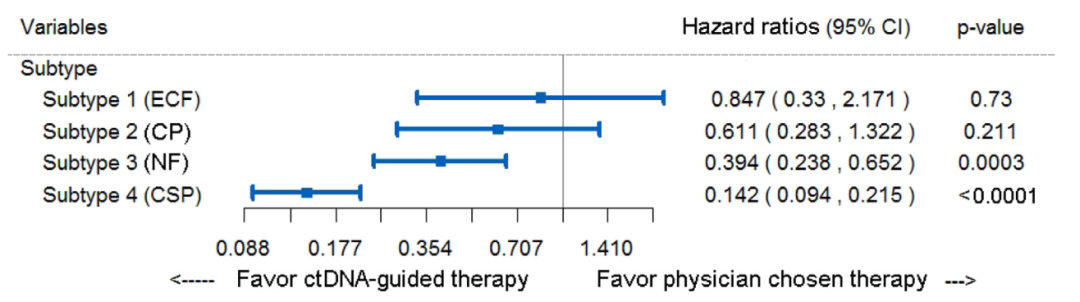
图6. 基于ctDNA亚型的无进展生存风险比亚组分析
研究结论
本网站所有内容来源注明为“梅斯医学”或“MedSci原创”的文字、图片和音视频资料,版权均属于梅斯医学所有。非经授权,任何媒体、网站或个人不得转载,授权转载时须注明来源为“梅斯医学”。其它来源的文章系转载文章,或“梅斯号”自媒体发布的文章,仅系出于传递更多信息之目的,本站仅负责审核内容合规,其内容不代表本站立场,本站不负责内容的准确性和版权。如果存在侵权、或不希望被转载的媒体或个人可与我们联系,我们将立即进行删除处理。
在此留言







#多中心#
75
#真实世界#
78
#转移性#
65
#DNA突变#
63
学习
66
学习了#学习#
63
学习学习学习学习学习学习学习学习学习学习学习学习学习学习学习学习学习学习学习学习学习学习学习学习学习
60