晕厥不能忽视“罕见病”!
2020-06-30 小可爱 医学之声

晕厥是由于短暂的全脑低灌注导致的短暂意识丧失(Transient loss of consciousness,T-LOC),特点为发生迅速、短暂、自限性、并能够完全恢复的意识丧失。
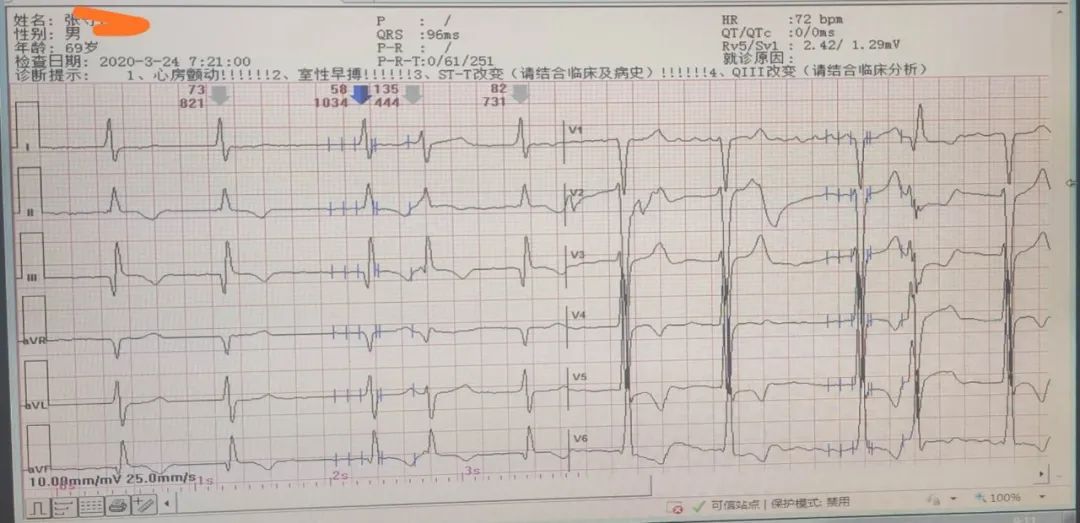
晕厥是由于短暂的全脑低灌注导致的短暂意识丧失(Transient loss of consciousness,T-LOC),特点为发生迅速、短暂、自限性、并能够完全恢复的意识丧失。有较高的发病率、致残率及致死率,在普通人群中并非少见,约占35%。导致晕厥的病因很多,机制复杂,涉及多个学科,且临床表现复杂且缺乏特异性,可与多种疾病表现类似,给医生的早期临床诊断带来了困难。 最重要的病因包括心源性、神经源性和代谢紊乱以及药物副作用。其中心源性晕厥最常见,病因包括心脏瓣膜病、急性心肌梗死/缺血、梗阻型心肌病、心包疾病/心脏压塞、先天性冠状动脉异常、人工瓣膜异常。通过这篇文章,我们讨论心源性晕厥罕见病因左心房粘液瘤的临床表现,诊断、治疗。 病例报告如下 患者,男性,27岁,以“两次晕厥”为主诉入我院急诊科,病程中无发热、咳嗽、咳痰、咯血、盗汗、胸痛、胸闷、呼吸困难、气短等不适。无高血压、冠心病、糖尿病、脑梗死等既往病史,无吸烟、饮酒史。 急诊科查体:血压:129/75mmHg,心率:75次/分,呼吸:18次/分,体温:36.5℃,氧饱和度:99%,心脏可闻异常心音(S1较强),奇怪的是心尖部收缩期及舒张期可闻及杂音,杂音强度不定,随体位变化而明显变化,颈静脉充盈及怒张(-)。其余系统检查(包括神经学检查)均未见明显异常。 辅助检查:实验室检查结果均未见明显异常,心电图提示:窦性心律,头颅核磁及胸片均未见明显异常,心脏彩超:显示:一个较大的高回声病灶,其内有清晰可见的源自左心房(LA)柄状结构(如图所示)。 因此,患者被转移到心脏外科中心进行外科,在全麻体外循环下行“左房粘液瘤摘除术”,术中见左房粘液瘤为7×6cm大小。 术后患者恢复良好,2周后出院。术后定期随访无任何不适。 讨论 心源性晕厥可由心房粘液瘤所致的流出道梗阻引起,心房粘液瘤是导致猝死的最常见的原发性心脏肿瘤,以30至60岁女性常见。由于乏力、晕厥等非特异性症状,并且临床症状因肿瘤在心房/心室的位置不同而异,故早期诊断可能较困难。在不同病例中,心房是主要受累的心腔,粘液瘤常位于左心房。 心房粘液瘤早期因起病隐匿,不易发现,临床上易出现漏诊,需引起重视。呼吸困难通常是最常见的症状,Prousi等报道长期心悸等非特异性症状也是常见的临床症状。Torregrossa等报道,61岁男性患者,有慢性咳嗽及双侧下肢浮肿病史1年,经急诊超生检查后诊断为心房粘液瘤。本例特点是患者年轻,且病情急性发作。Mathew 等报告心房粘液瘤另一种罕见的特点是18岁女性患者出现双侧肢体急性缺血的临床表现。 超声心动图是诊断心房粘液瘤的首选方法。Raja Rao等研究表明,尽管临床表现多种多样,但经床旁超声和超声心动图评估对急诊科疑似病例可能是有益的。在这种情况下,在腔内具有移动的肿块可能提示为粘液瘤或血栓。虽然临床表现多种多样,手术治疗方式也各不同,但最终的远期预后一般情况下良好的,无明显不良后果,但也有关于术后死亡结局及复发的报道。 结论 总之,强调的是急诊科医师应该熟悉心脏肿瘤的非特异性临床表现,以改善粘液瘤患者的最终结果,充分利用床旁超声进行及时诊断,临床上一旦诊断心房粘液瘤,应行手术治疗,后续的治疗至关重要。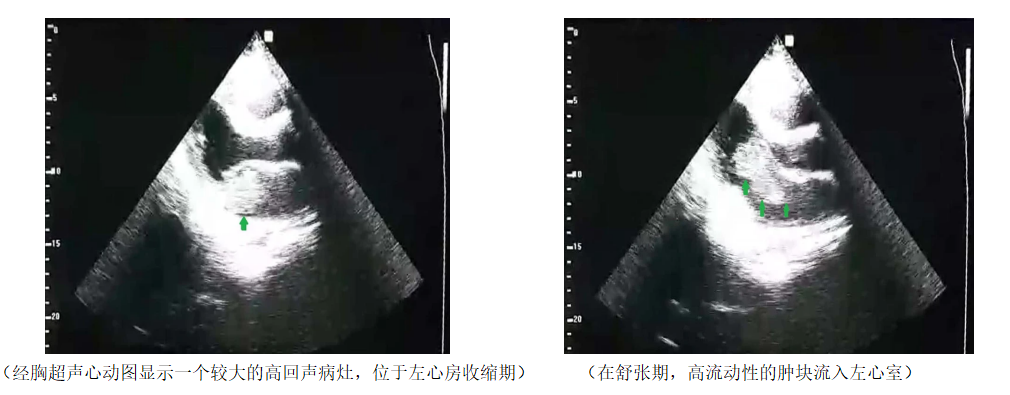
本网站所有内容来源注明为“梅斯医学”或“MedSci原创”的文字、图片和音视频资料,版权均属于梅斯医学所有。非经授权,任何媒体、网站或个人不得转载,授权转载时须注明来源为“梅斯医学”。其它来源的文章系转载文章,或“梅斯号”自媒体发布的文章,仅系出于传递更多信息之目的,本站仅负责审核内容合规,其内容不代表本站立场,本站不负责内容的准确性和版权。如果存在侵权、或不希望被转载的媒体或个人可与我们联系,我们将立即进行删除处理。
在此留言








越简单越复杂
119
#晕厥#
90
#罕见#
88
😐️
150