

背景
大剂量局麻药可造成更大范围的感觉阻滞,但风险也更大。本试验的目的是比较接受乳房手术的患者在前锯肌深平面注射不同体积罗哌卡因的效果。
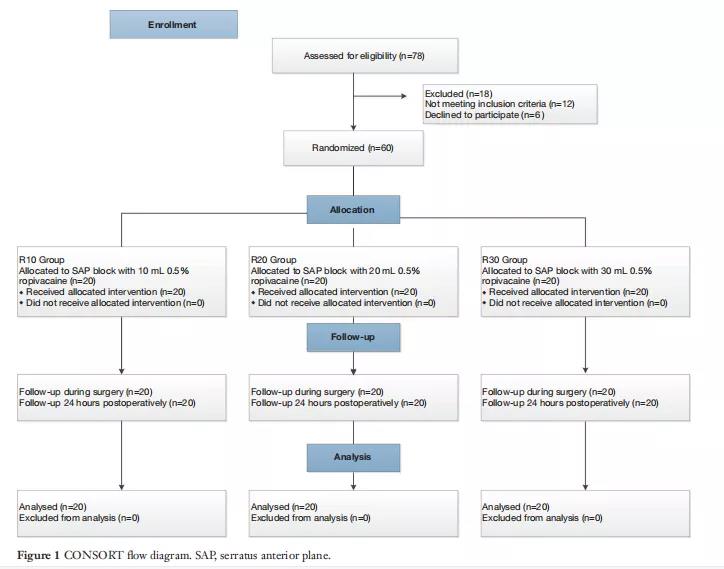
方法
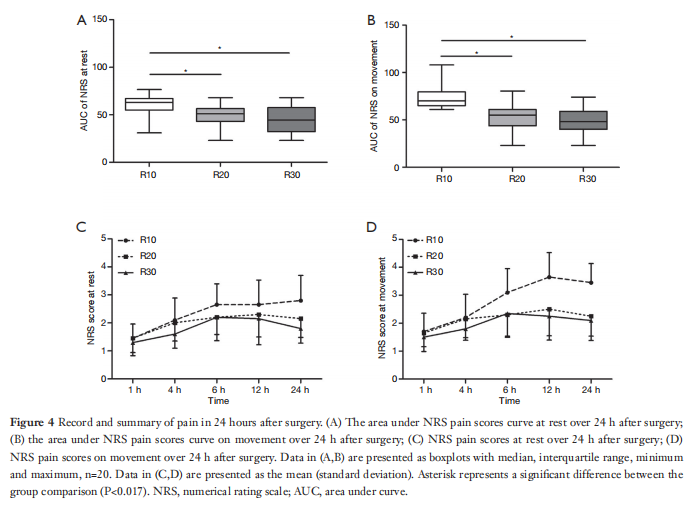
在这项随机双盲试验中,60例接受乳腺手术的患者被随机分为R10、R20和R30组(n=20),分别接受10、20和30mL 0.5%罗哌卡因的深锯前平面阻滞。阻滞30分钟后,沿腋中线沿颅尾方向冷刺激测试皮肤感觉。记录术后24小时内疼痛数值评分,并通过数字评分量表疼痛评分估计曲线下面积。并记录了抢救镇痛的病例和不良事件的发生率。
结果
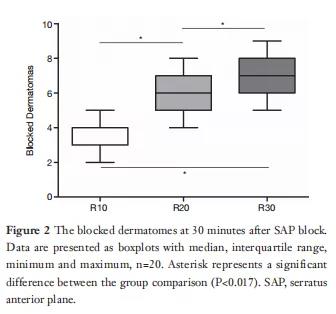
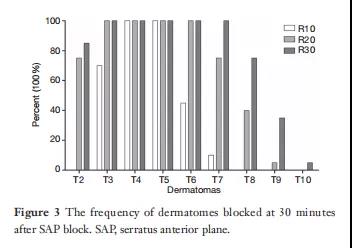
R10组、R20组和R30组的阻滞皮肤范围分别为3[3,4]、6[5,7]和7[6,8](R10组与R20组比较,P<0.001;R10与R30比较,P<0.001;R20对R30,P=0.005)。R10组的曲线下面积明显高于R20和R30组(静止时P=0.014,P=0.003;运动时,P<0.001,P<0.001)。

结论
当使用10、20和30ml罗哌卡因进行深锯肌前平面阻滞时,阻滞的皮肤随着容量的增加而增加。20和30毫升的镇痛效果相似,优于10毫升。因此,在乳房手术中,20毫升罗哌卡因的容量被认为适合于深锯齿前平面阻滞。
原始出处:
Kejian Shi, Ying Chen, Le Liu,et al.Comparison of the effect of different volumes ropivacaine on deep serratus anterior plane block in patients undergoing breast surgery: a prospective randomized double-blinded trial.[J] Ann Palliat Med 2021;10(6):6104-6111.
本网站所有内容来源注明为“梅斯医学”或“MedSci原创”的文字、图片和音视频资料,版权均属于梅斯医学所有。非经授权,任何媒体、网站或个人不得转载,授权转载时须注明来源为“梅斯医学”。其它来源的文章系转载文章,或“梅斯号”自媒体发布的文章,仅系出于传递更多信息之目的,本站仅负责审核内容合规,其内容不代表本站立场,本站不负责内容的准确性和版权。如果存在侵权、或不希望被转载的媒体或个人可与我们联系,我们将立即进行删除处理。
在此留言




#前瞻性#
56
#ALL#
64
#罗哌卡因#
72
#双盲#
64
#Med#
43
学习了
67
高质量研究,读起来真爽,谢谢梅斯
84
疗效只是效果的众多方面之一,还要看对患者的获益,包括生活质量等因素共同决定效果的
73