
Infection: 入住重症监护病房的COVID-19患者与菌血症相关的危险因素分析
2022-06-21 xuyihan MedSci原创

菌血症指致病菌由局部侵入血流,但未在血流中生长繁殖,只是短暂的一过性通过血液循环到达体内适宜部位后再进行繁殖而致病。一般来说,导尿管或者是体表的手术造口容易导致发生菌血症。
SARS-CoV-2病毒已导致卫生系统面临最大的挑战。尽管大多数新冠患者的病例临床过程是轻微的,但15%的患者会发展为严重疾病,并且由于呼吸衰竭需要进入重症监护室 (ICU) 并需要呼吸机支持治疗。事实上许多研究表明,多达24%的住院COVID-19患者报告了细菌和真菌双重感染,而且比例明显增加。与未感染的患者相比,COVID-19患者的血流感染 (BSI) 发生率较高,并且 BSI的发展与较差的结果相关。本项研究的目的是评估ICU中 COVID-19阳性患者中发生 BSI 的风险因素。特别是评估了免疫抑制治疗对 BSI 风险的影响。
本项研究招募了2020年2月至2021年2月间在意大利两家不同医院的 COVID-19 专用 ICU收治的所有COVID-19 患者。所有成年COVID-19 患者入住ICU ≥ 48小时。主要观察终点是因COVID-19入住ICU期间BSI发作的频率,即在ICU入院后≥48小时被诊断为 ICU 获得性菌血症,则将其定义为 BSI。
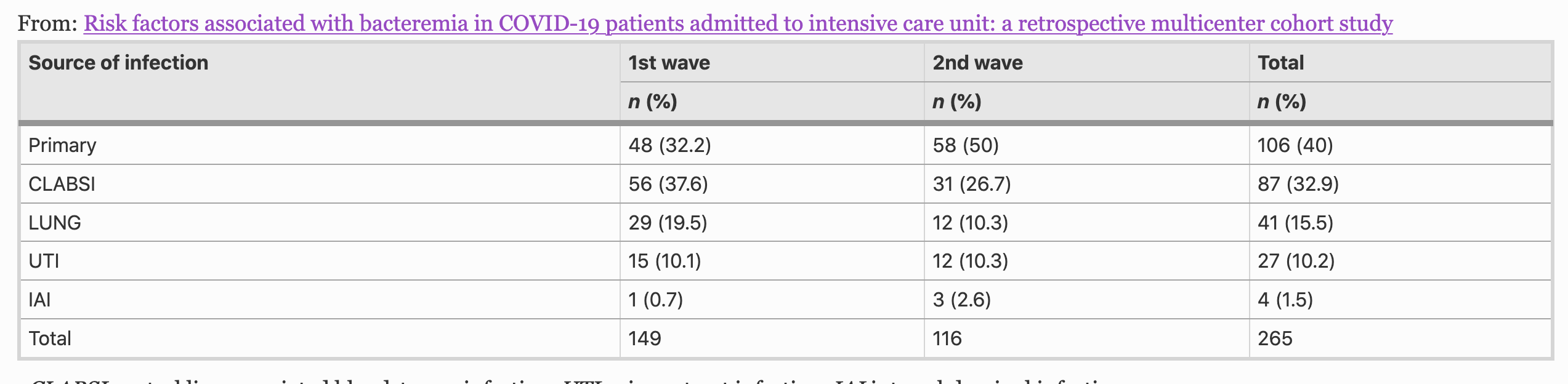
研究结果显示本项试验共包括537名患者,其中265名 (49.3%) 经历了至少一次BSI。发生菌血症的患者SOFA评分较高[10 (8-12) vs 9 (7-10),p < 0.001],插管频率更高 [95.8% vs 75%,p < 0.001],中位时间更长时间 [16天 (9-25) VS 8天 (5-14),p < 0.001]。与未发生 BSI 的患者相比,患有 BSI 的患者的 ICU 停留时间中位数更长 [18 天 (12-31.5) VS 9 天 (5-15),p < 0.001] 和更高的死亡率 [54% VS 42.3%,p < 0.001]它。BSI 的发展导致更高的 SOFA 评分 [aHR 1.08 (95% CI 1.03–1.12)] 和更高的 Charlson 评分 [csAHR 1.15 (95% CI 1.05–1.25)]。
本项研究证实在ICU中治疗的患者出现高SOFA分数和高 Charlson 分数与 BSI 的发展相关。相反,类固醇和托珠单抗等免疫抑制疗法不会增加菌血症的风险。
原始出处:
Cecilia Bonazzetti. Et al. Risk factors associated with bacteremia in COVID-19 patients admitted to intensive care unit: a retrospective multicenter cohort study. Infection.2022.
本网站所有内容来源注明为“梅斯医学”或“MedSci原创”的文字、图片和音视频资料,版权均属于梅斯医学所有。非经授权,任何媒体、网站或个人不得转载,授权转载时须注明来源为“梅斯医学”。其它来源的文章系转载文章,或“梅斯号”自媒体发布的文章,仅系出于传递更多信息之目的,本站仅负责审核内容合规,其内容不代表本站立场,本站不负责内容的准确性和版权。如果存在侵权、或不希望被转载的媒体或个人可与我们联系,我们将立即进行删除处理。
在此留言









#COVID-19患者#
72
#菌血症#
55
#重症监护病房#
87
#Infection#
0
#监护#
65
好文章,谢谢分享。
67