
入住重症监护病房 (ICU) 的结缔组织疾病患者的脓毒症死亡率很高
2022-02-15 SNOW MedSci原创

系统性红斑狼疮 (SLE) 等结缔组织疾病 (CTD) 患者感染的风险增加。本研究调查了在重症监护室 (ICU) 治疗脓毒症的 CTD 患者的结果和特征。
进行单中心回顾性分析,回顾2006年至2019年间某大学医院ICU因脓毒症收治的所有CTD诊断患者。计算死亡率,采用多因素logistic回归检测脓毒症死亡率的独立危险因素. 此外,评估了 ICU 评分如序贯器官衰竭评估 (SOFA) 评分的阳性预测值。
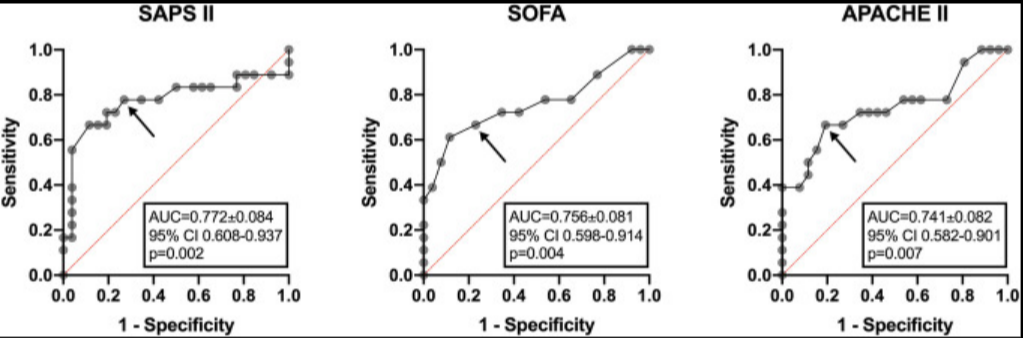
SOFA、SAPS II 和 APACHE II 评分在预测住院死亡率方面的接受者操作特征 (ROC) 分析。曲线下面积 (AUC) 以标准误差 (±SE)、95% 置信区间 (CI) 和 p 值显示。箭头显示了预测高概率死亡率的合理截止值,如下所示:SAPS II = 47(特异性 73%,敏感性 78%),SOFA = 9(特异性 77%,敏感性 67%),APACHE II = 31(特异性 81 %,灵敏度 67%)。APACHE II,急性生理学和慢性健康评估 II;AUC,曲线下面积;CI,置信区间;SAPS II,简化的急性生理评分 II;SOFA,顺序器官衰竭评估。
本研究包括 44 名 CTD 患者(平均年龄 59.8 ± 16.1 岁,68.2% 为女性),其中大多数被诊断为 SLE(61.4%),其次是系统性硬化症(15.9%)。56.8% (n = 25) 接受免疫抑制剂治疗,81.8% (n = 36) 接受糖皮质激素治疗。3 名患者 (6.8%) 使用了利妥昔单抗。脓毒症CTD患者的住院死亡率高达40.9%。它在系统性硬化症(SSc)患者中最高(85.7%)。在多元逻辑回归中,SOFA 评分和 SSc 诊断与死亡率独立相关(P= 0.004 和 0.03,分别)。简化的急性生理学评分 II (SAPS II)、SOFA 和急性生理学和慢性健康评估 II (APACHE II) 评分是研究队列中败血症死亡率的良好预测指标(SAPS II AUC 0.772,P = 0.002;SOFA AUC 0.756,P = 0.004;APACHE II AUC 0.741,P = 0.007)。
结论: CTD患者院内脓毒症死亡率较高。SSc 诊断和 SOFA 与死亡率独立相关。此外,常见的 ICU 评分是死亡率的良好预测指标。
原文:Krasselt M, Baerwald C, Petros S, Seifert O. Sepsis Mortality Is high in Patients With Connective Tissue Diseases Admitted to the Intensive Care Unit (ICU). J Intensive Care Med. 2022 Mar;37(3):401-407.
本网站所有内容来源注明为“梅斯医学”或“MedSci原创”的文字、图片和音视频资料,版权均属于梅斯医学所有。非经授权,任何媒体、网站或个人不得转载,授权转载时须注明来源为“梅斯医学”。其它来源的文章系转载文章,或“梅斯号”自媒体发布的文章,仅系出于传递更多信息之目的,本站仅负责审核内容合规,其内容不代表本站立场,本站不负责内容的准确性和版权。如果存在侵权、或不希望被转载的媒体或个人可与我们联系,我们将立即进行删除处理。
在此留言










#结缔组织#
80
#疾病患者#
67
#重症监护病房#
78
#监护#
83
学习了
88